Cervical cancer is a cancer
that starts in the cervix (the lower part of womb). It can spread to adjacent
structures such as vagina, pelvic organs and then to distant organs e.g.
liver, lung or brain.
The proven way to
prevent cervix cancer is to have regular testing (screening) to find
pre-cancers, as it takes several years before they can turn into invasive
cervical cancer. The cervical smear is the screening test to detect for early
pre-cancer change, which can be well treated before cancer develops. HPV
vaccine is also a proven effective preventive method.
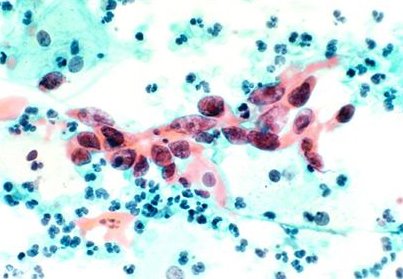
A cervical smear is a
sample of cells from the outside of the cervix (or neck of the womb) that
allows detection of pre-cancerous abnormalities of the cervix. It is simply a
screening tool, which indicates that more investigation should be considered
at the cervix.
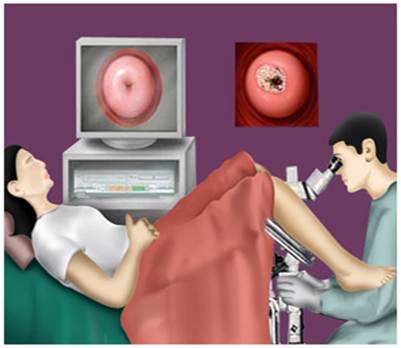
Colposcopy is a more
detailed examination of the cervix. Instead of looking at the cervix with the
naked eye, a special magnifying binoculars is used to see the changes at high
magnification. Sometimes a picture is taken for comparison in the future for
the progress. The examination may take a little longer than a standard smear
test.
Pre-cancerous changes are
also called Cervical Intraepithelial Neoplasia (CIN). The main treatment
option for CIN is LLETZ (Large Loop Excision of the Transformation Zone).
Laser can be used to cut the cone as an alternative to LLETZ. All treatment
methods are effective.
It is a very common
virus that comprises of about 200 types. The most well known type is probably
the one that causes common warts, commonly found on the hands and feet. There
are about 30 types of HPV affecting the genital area; these include both the
'low risk' and the 'high risk' HPV types. The low risk HPVs sometimes cause
genital warts but they do not cause cervical cancer. In contrast, the high
risk HPVs may cause abnormal cellular changes in the uterine cervix, called
'cervical intraepithelial neoplasia ("CIN")'. While low grade CIN
may sometimes regress, high grade CIN may eventually develop into cervical
cancer if appropriate treatment is not given.
Yes. According to
studies on young female in UK and USA, including college students, around 50%
will be infected by HPV within 5 years after sexual experience, even with a
single partner.
According to studies in
the US Centers for Disease Control, the lifetime risk of HPV infection is at
least 50% among sexually active men and women. About 70% of new cases with HPV
infections, including those with the high-risk HPV types will regress within
one year. CIN and cervical cancer will only develop in a portion of women
with persistent infection by high-risk HPV types. HPV is therefore a
necessary, but not the only factor for the development of cervical cancer.
Since almost all cases
of cervical cancer are caused by HPV infection, protection against HPV
infection will naturally protect women from cervical cancer. The majority of
HPV vaccines available today offers more than 90% protection for women
against infection with HPV type 16 and 18, which are the two types of high
risk HPV that cause approximately 70% of cervical cancer throughout the
world. So the vaccine cannot protect 100% against cervical cancer. Although
it offers very good protection against 70% of the cervical cancer, there are
still 30% not covered by the vaccine.
The HPV vaccines
available currently, or in the near future, are for prophylaxis only. In
other words, they are useful for protecting women from HPV infection and
cannot be used to cure current HPV infection.
Since these vaccines
are for prophylaxis, ideally they should be given before exposure to HPV infection,
i.e. before sexual exposure. However, it may still offer protection if you
have sexual exposure because the degree of protection varies depending on
whether there had been prior infection with HPV16 and/or HPV18 at the time of
vaccination.
No, since the current vaccines
could only provide 70% protection against cervical cancers which are caused
by HPV types 16 and 18, one could still be infected with other high risk HPV
types that also cause cervical cancer. Perhaps, there may be a need for
modification of the screening programme in future but it is currently too
early to comment.
According to the current
data on clinical trials, no significant serious side effects have been
encountered. However, mild to moderate pain and redness at the sites of
intramuscular injection may develop, similar to vaccination against other
diseases. Occasionally, fever was reported as a systemic side effect.
No conclusive data is available
at the moment. While preliminary data did not reveal any significant adverse
effect on pregnancy and infant, women are advised to adopt contraception till
the completion of the three doses of vaccines.
Most clinical studies
show that the HPV vaccines are safe. The manufacturers use empty viral
particles to make the viral like particles as to induce immune response in
host. In another words, one would not find live virus or viral DNA inside the
vaccine.
The minor side effects
that may associate with the vaccines include fever, headache, swelling over
the site of injection. Most of the above are usually mild.
Some studies claim
girls of around 9 to 10 years old are ready to have the injection. It is best
to have the vaccine before one acquire the HPV virus. The Joint Committee for
Vaccination and Immunization in UK recommended routine vaccination for girls
aged around 12-13 years after they conducted a detailed review on HPV
vaccination.
If one have severe
allergic reaction or hypersensitivity to yeast or to any component contained
in the vaccine, she should not have the vaccination. For those who have high grade
fever and those who are pregnant also best to postponed the injection.
No. Cervical smear is
not necessary before the vaccine administration. However, regular cervical
screening is still recommended even after vaccination.